FIRST SEMESTER PRODUCTS OF CONCEPTION:
- Grossly small amount of tissue (tissue minus blood <4 -5cm).
- Villi are small (size of 2-2.5 endometrial glands or <4 mm) (figure 1).
- Trophoblastic proliferation in polarized (trophoblasts grow in columns towards the oxygen source)

Exceptions: extrauterine (fallopian tube pregnancy) can show significant trophoblastic proliferation. This can be attributed to the more circumferential oxygen source in a very tight space and generally earlier gestational age in tubal pregnancies. (figure 2).
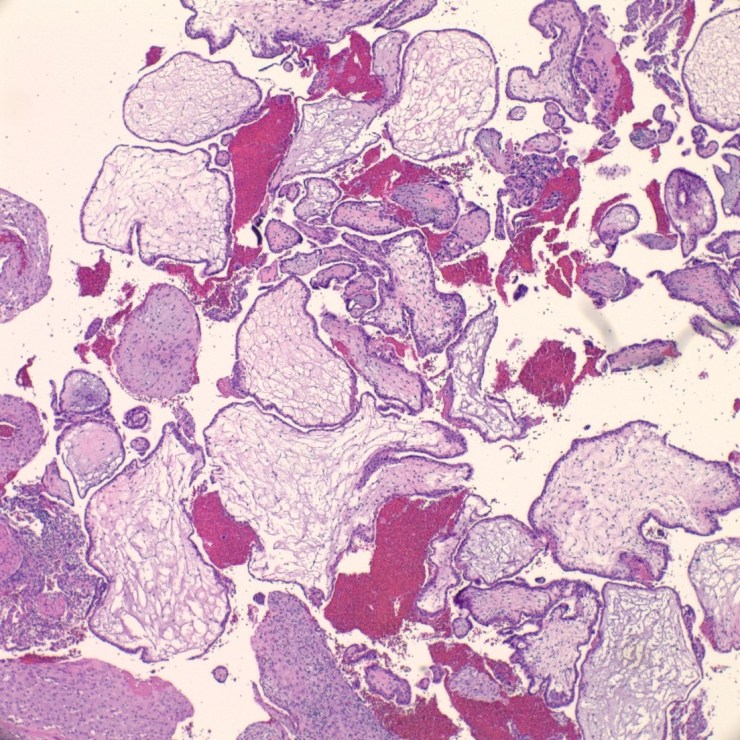
COMPLETE HYDATIDIFORM MOLES:
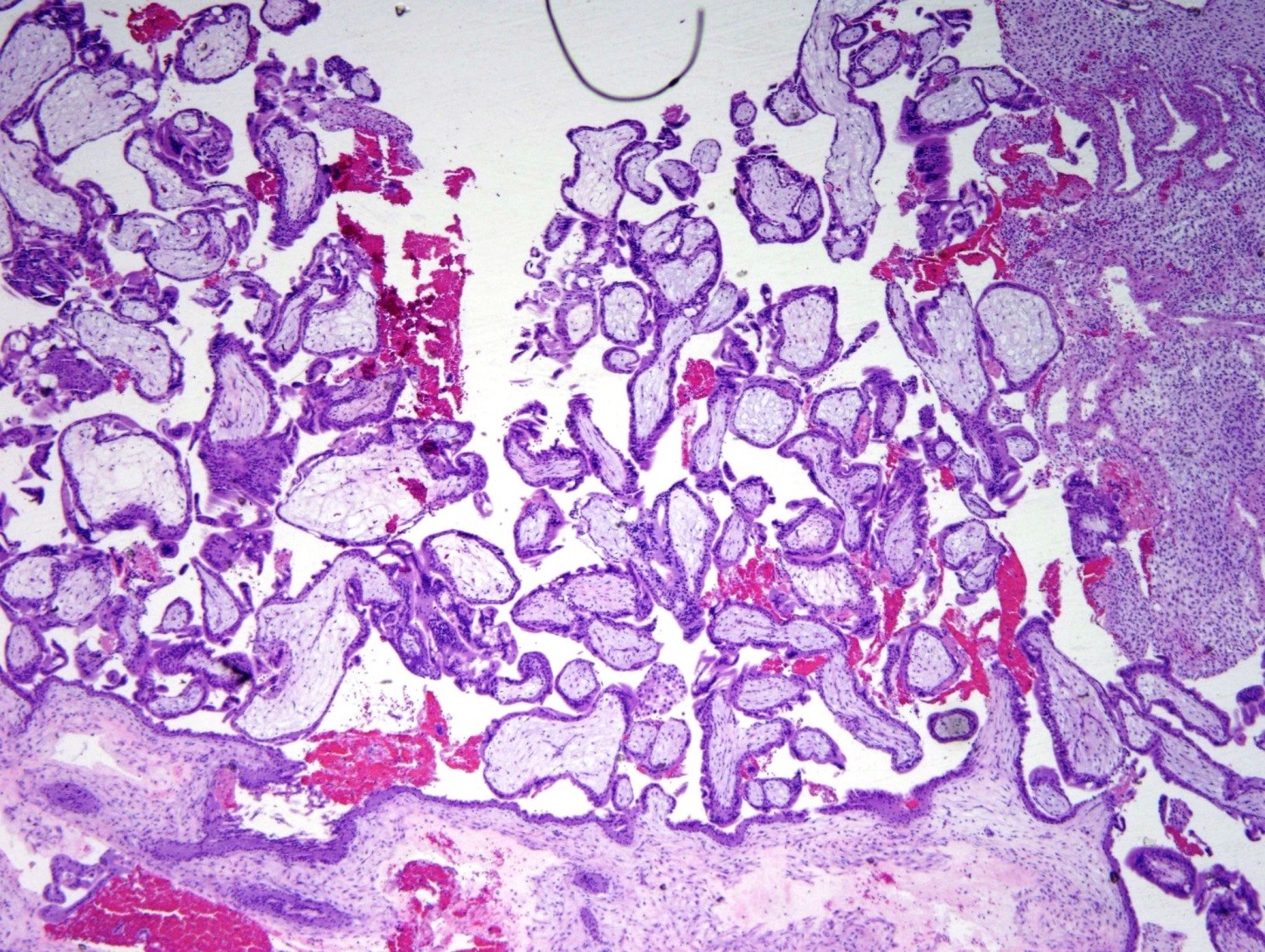
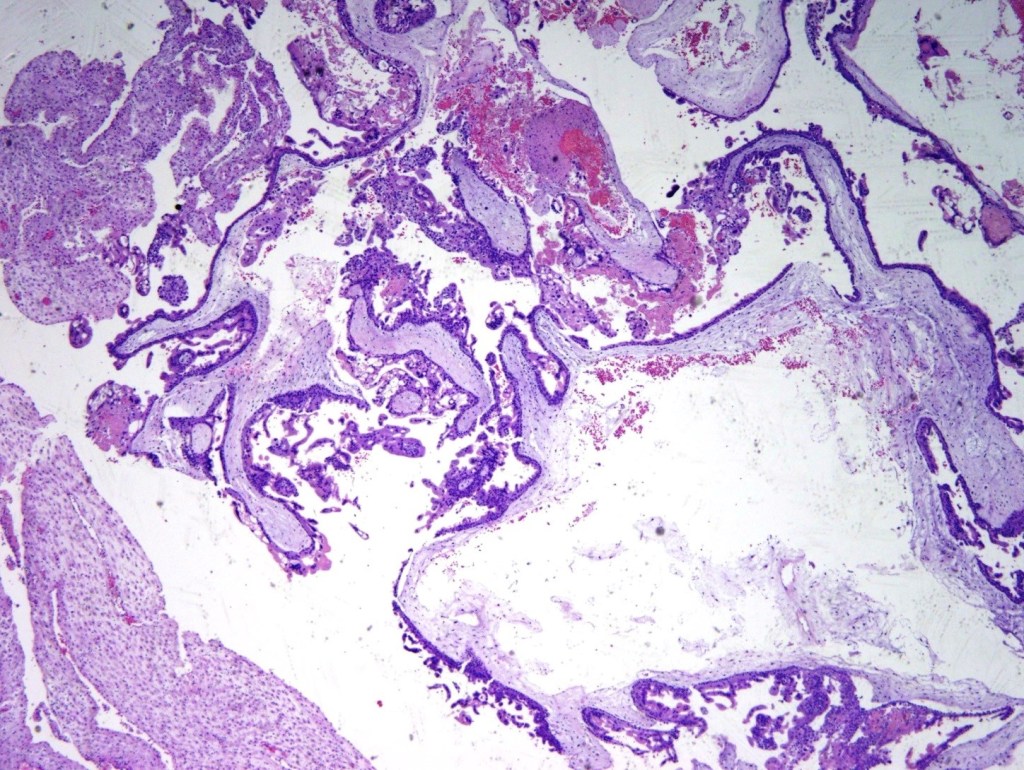
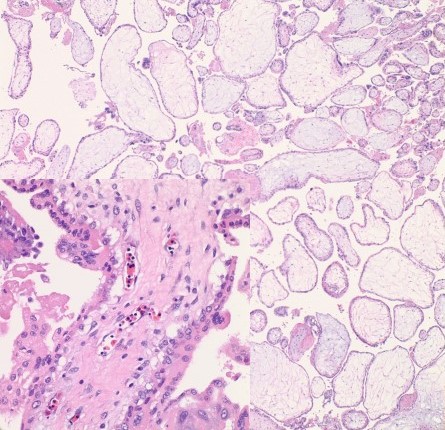
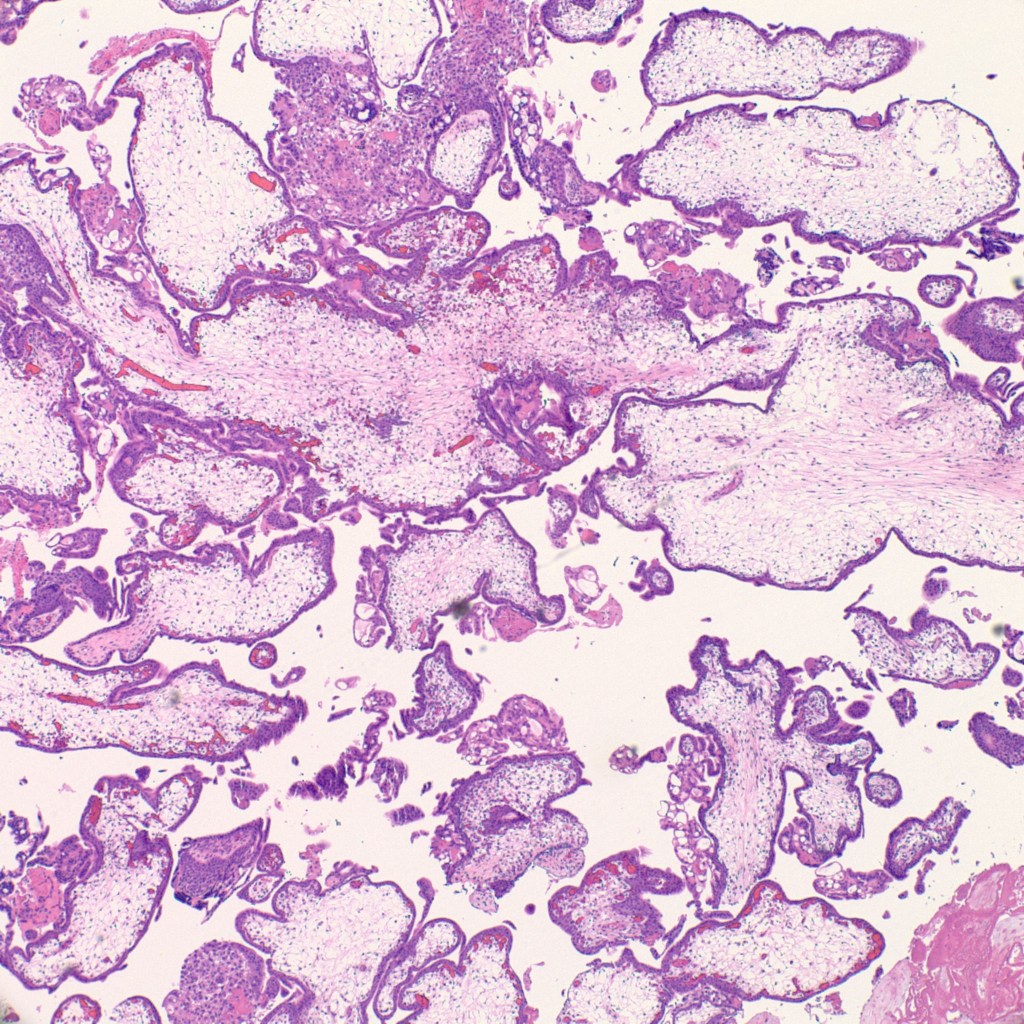
- Grossly large amount of tissue (5 cm and more) with sometimes large ballooned villi (>1 cm).
- Presence of cisterns, circumferential or almost circumferential trophoblastic proliferation and trophoblastic inclusions (figure 3-4).
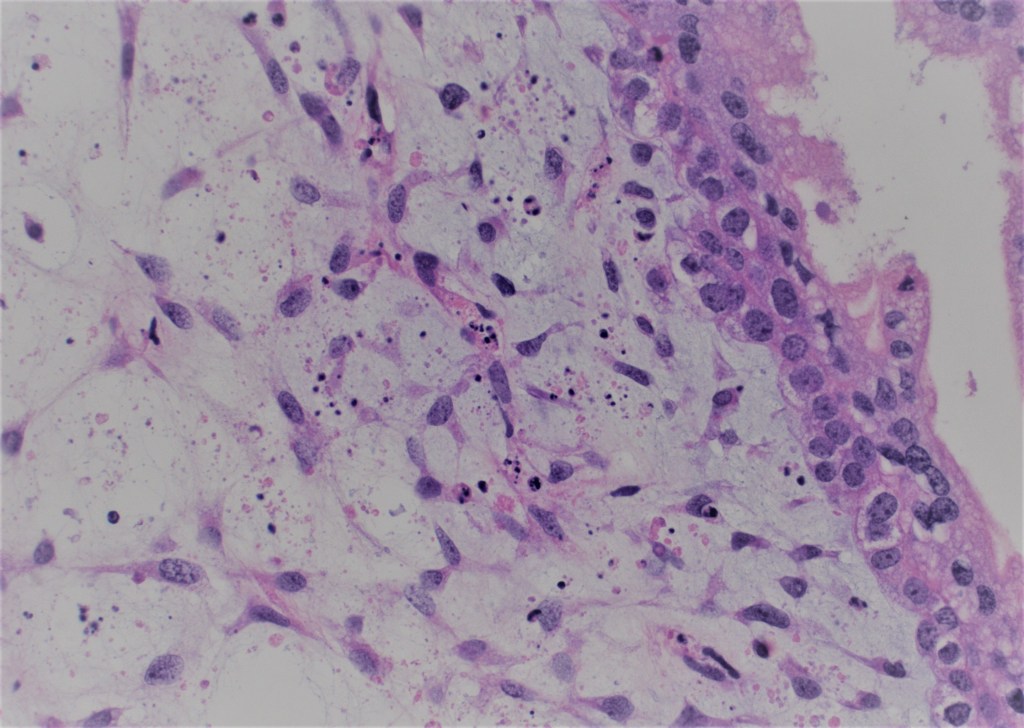
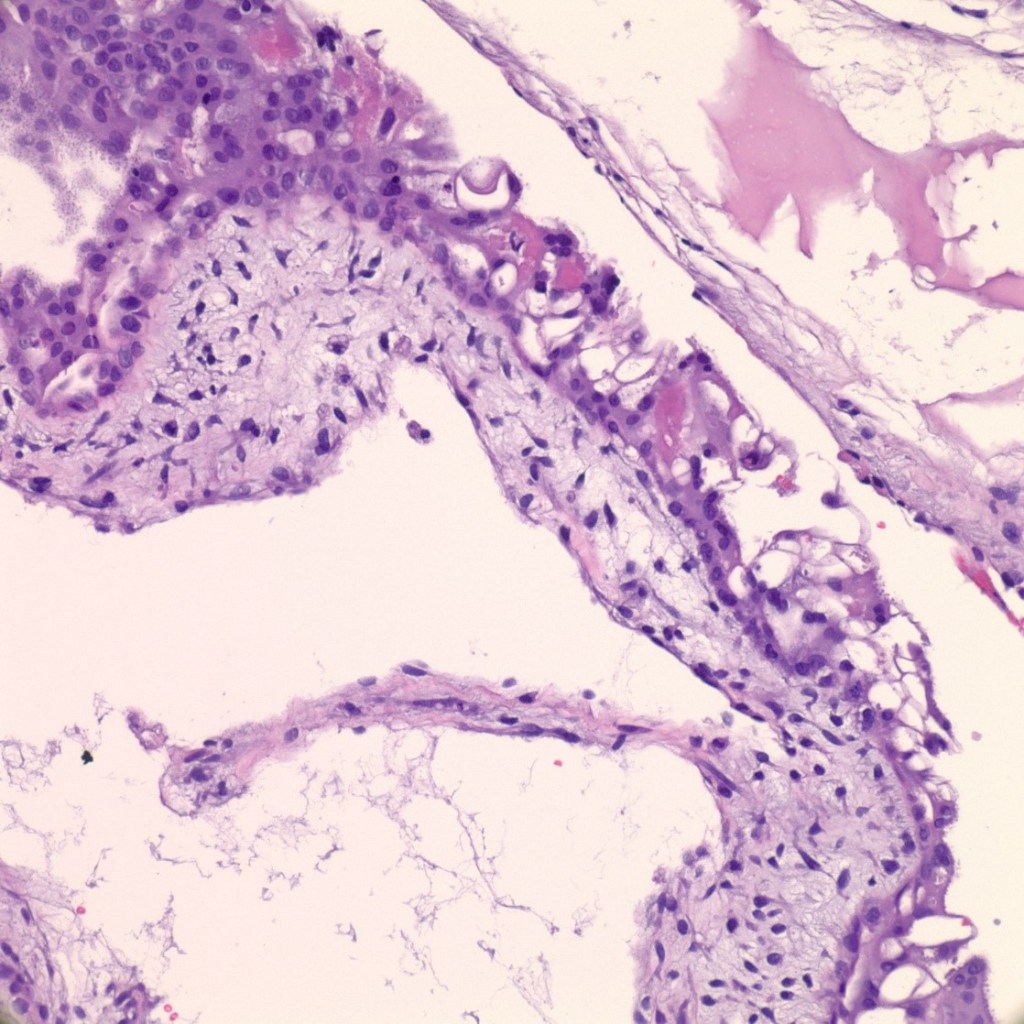
- Blue myxoid stroma with karyorrhexis (figure 5).
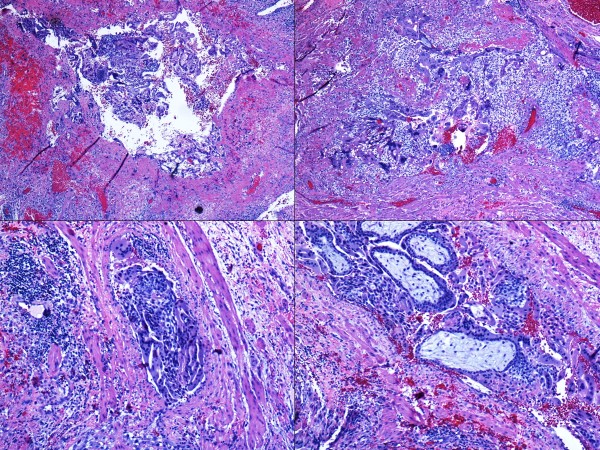
- Atypical and exaggerated implantation site with large trophoblasts, at least three times larger than decidual cells (figure 6).
- 99.9% of the time there is no fetus and no nucleated red blood cells in the villi.
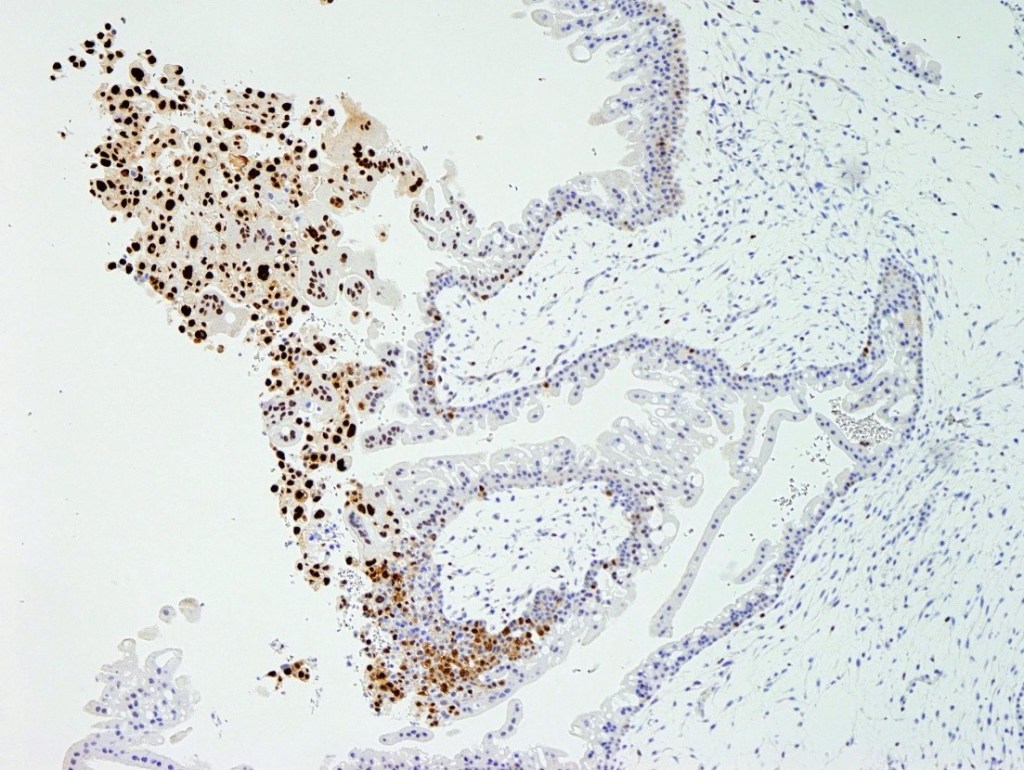
- P57 (maternally expressed paternally imprinted) is negative in the villous stroma and trophoblasts (figure 7).
- Cytogenetics or DNA ploidy studies: diploid or tetraploid-paternal chromosomes only. The theory includes fertilization of an empty ovum with one sperm with subsequent duplication (so-called “homozygous”) in 80-90 %of the cases. The second option is dispermic fertilization of an empty ovum (so-called “heterozygous”); 10-20 % of the cases and likelihood to be associated with a persistent molar pregnancy.
- Rare case reports reported the presence of fetus with complete mole


Differential diagnosis: hydropic abortion comes frequently in the differential diagnosis with a very early complete mole. Very early complete mole can have no trophoblastic proliferation, with or without a hint of cisterns. Blue stroma can look similar in both. Very early hydatidiform moles can show only irregular contours in a form of clubbing. In hydropic abortions, nucleated red blood cells are often present in the villi and they are an excellent clue (figure 8). I recommend having a low threshold for p57 immunohistochemistry in early abortions.
PARTIAL HYDATIDIFORM MOLES:
- Grossly moderate amount of tissue.
- Well-developed hydropic villi may not be obvious.
- Microscopically challenging diagnosis.
- The low-power view reveals a mix of small fibrotic villi and larger villi (figure 9).
- Some trophoblastic proliferation (in lace-like pattern) can be seen (figure 10).
- Embryo or fetus can be present.
- A limited number of cisterns are many times appreciated.
- Immunohistochemistry for p57 is positive.
- Cytogenetics or DNA ploidy studies: triploid (two paternal and one maternal set of chromosomes) or less likely tetraploid (three paternal and one maternal set of chromosomes).
Differential diagnosis: very early complete hydatidiform mole or chromosomal abnormalities such as trisomies (figure 10).
The most accurate ancillary test is DNA genotyping
Molar pregnancies have a risk of persistent gestational trophoblastic disease. The percentages are higher in complete (about 20%) than partial moles (<5%). There is also a small risk of gestational choriocarcinoma arising from molar pregnancies.
Clinical follow-up includes ensuring that B-Hcg level reaches zero and stays zero (most often 6 months follow-up).
USEFUL TIPS:
- Beware of overdiagnosing molar pregnancies in the fallopian tube.
- In early pregnancy exuberant trophoblastic proliferation can be seen but if possible submit the entire material and cut levels to find villi. If villi are not present always consider non-villous gestational trophoblastic disease.
- An early complete mole can be easily missed-look for nucleated red blood cells in the villi or have a low-threshold to order p57.
